DATA ALIGNMENT FOR COMBATING HIV/AIDS
The United States President's Emergency Plan for AIDS Relief (PEPFAR) is a commitment by the United States Government to support HIV/AIDS prevention, care and treatment programs in developing countries. Kenyans living with HIV/AIDS get treatment thanks to this initiative.
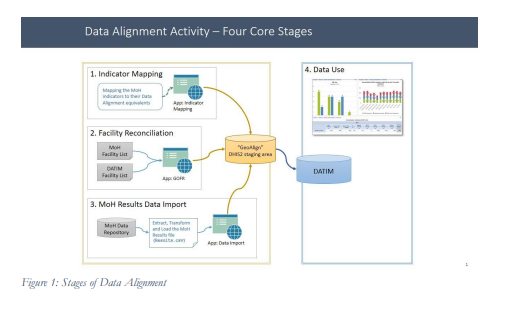
The program established Data for Accountability, Transparency and Impact Monitoring (DATIM), to help save the lives of those suffering from HIV/AIDS around the world by collecting AIDS data to analyze PEPFAR program effectiveness and efficiency and to help improve accountability and decision making. DATIM is the PEPFAR-specific version of Kenya Health Information System (KHIS) in Kenya. KHIS is customized from DHIS2, an open-source software platform for reporting, analysis and dissemination of data for all health programs, developed by the Health Information Systems Program, University of Oslo and is used to collect data at all levels required for; site level reporting at the facility and community level as well as aggregations at the subnational and national levels in Kenya
Although the data that feeds DATIM and KHIS come from the same source document in the facilities, the same data in both platforms is different. The assumption is that the errors occur in transmission and collation. A source at National AIDS and STI Control Programme (NASCOP) the programme that is responsible for HIV data says
There was differences in the numbers found in DATIM and KHIS, even though the source documents the facility level were the same, we needed to find out why this was happening and correct it.
The need for concordance between the data in KHIS and DATIM to eventually have one central source of information on HIV, led to the roll-out of Data Alignment Activities (DAA) at the national level, county level especially HIV prevalent counties such as Homabay, Kisumu, Siaya, Migori and Busia among others and at the institutional level. The main focus for the data alignment activity is to strengthen the government system for reporting Health Information Systems (HIS) in such a way that it becomes the single source of information both for government, partners and donors.
HealthIT is a USAID funded activity whose goal is to contribute towards enhancing evidence-based decision making by all health sector stakeholders through leveraging and strengthening integrated Health Information Systems. The activity supports the Ministry of Health’s National AIDS and STI Control Programme (NASCOP) to compare data reported in DATIM and the data in Kenya Health Information System (KHIS) through the data alignment activities. DATIM is managed by PEPFAR globally and all the implementing mechanisms report to it and the data reported to KHIS is reported by the HRIOs at different levels from national to facilities. Then there is data that goes to both DATIM and KHIS, the facility level data collection tools such as the registers and the forms. The source of the data going to DATIM is from the MOH-731data collection form and is the same source of data that goes to KHIS.
According to PEPFAR, the data alignment activity is meant to provide a comprehensive view of national programs to understand the full HIV landscape to help define targeted interventions in both the longterm where the activity is meant to derive PEPFAR data directly from Ministry of Health (MOH) systems to reduce duplicative data entry and parallel reporting structures, thereby strengthening MOH systems to effectively monitor and maintain epidemic control and facilitate systems interoperability and in the shortterm where countries will use the data to identify reporting challenges, with the goal to improve reporting processes, data quality, and program efficiencies.
USAID’s HealthIT offers technical support to counties and partners working with NASCOP as they strive towards improving concordance between the two systems. HealthIT’s scope is to also support NASCOP review the indicators for mapping, facility issues, as sometimes there is a need to merge the facilities first before data is exchanged.
According to NASCOP, DAA is a very necessary intervention in aligning data in the two platforms used for decision making i.e., Kenya Health Information Systems (KHIS) and DATIM which is used by PEPFAR for reporting. What has been happening over time in the country is that the data collection tools have been trying to move to be consistent with what is in DATIM based on WHO guidelines but the process is near completion. In Kenya, data exchange has been done by way of course aggregate i.e., less than 15 years of age group, over 15 years of age group and comparing the same in DATIM.
DAA is an activity that harmonizes the two aggregate systems that are commonly used at the national level for a lot of decision making and also for monitoring of the progress of the HIV epidemic. What necessitated this was the difference in our numbers as our sources are common. For instance, our documents where the information is collected before aggregation to the aggregate system is the same, that at the facility level we use similar registers and similar reporting summary tools.- remarked the source
There are occasions when once the data had been aggregated and reported to the repository, there would be some variances from KHIS and DATIM. So DAA was basically to ensure that the difference between the data in the two systems was actually narrowed and when speaking of indicators, we are both speaking about the same indicator and we have a common understanding of its data capture process.
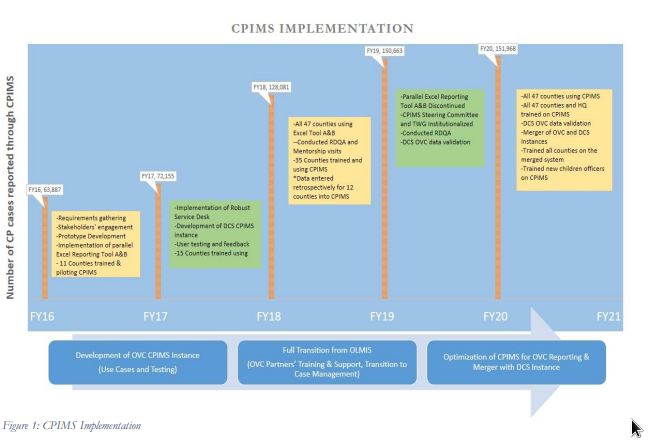
So far, USAID HealthIT has supported NASCOP conduct the DAA across 40 counties. At both the national and county levels, NASCOP says a key achievement and impact with the support of HealthIT has been being able to work on 7 out of the 9 key indicators that they commonly report on, capacity building to the counties as a way of building an understanding of some of the terminologies across the country. The indicators that they have been able to align include: PMTCT_ART (Number of HIV-positive pregnant women who received antiretroviral therapy (ART) to reduce the risk of mother-to-childtransmission during pregnancy), PMTCT_STAT (Number of pregnant women with known HIV status at antenatal care (includes those who already knew their HIV status prior to ANC), TX_NEW(Number of adults and children newly enrolled on antiretroviral therapy (ART),TX_CURR,(Number of adults and children currently receiving antiretroviral therapy (ART), among others. The data concordance in key Indicators included:
- TX_CURR ~ 99.47%
- TX_NEW ~ 98.21%,
- PMTCT_STAT ~ 97.96%,
- PMTCT_ART ~ 97.72%, and
- TB_PREV ~ 72.20%.
We all didn’t have a common understanding of how to calculate what is the current number of people living with HIV on ART and so we would have a different defined period and the gap from understanding of what to include when talking about treatment current. Are we including those who have missed their medicine for a month or those that are not to follow-up, and what is the definition of not to follow-up. But that has since changed- a representative from NASCOP Strategic Information added.
HealthIT has been instrumental in helping NASCOP, national and county partners to harmonize their terminologies, and they have been able to draw common data variables for both systems and this has really narrowed the gap in the numbers that are reported in the two platforms and that too is counted as an achievement.
The two indicators that are yet to be addressed are HTS-TST (Number of individuals who received HIV Testing Services (HTS) and received their test results) and TB-HIV (Number of adults and children on antiretroviral therapy (ART) who completed TB preventative therapy) and NASCOP is currently reviewing them by changing their tools to facilitate the capture of finer age-groups. The new tool for HTSTST will be released in October 2021 and the one for TB-HIV will be released after a meeting with the care and treatment team to discuss issues such as, who should be considered as a client who has completed Isoniazid Preventive Therapy because the challenge has been in capturing the number of clients who have completed the therapy. The meeting will enable all the stakeholders have a common understanding of this indicator.
HealthIT has also supported NASCOP in ensuring that they have a common understanding of the variables collected through the two systems. They have held trainings at both the national and county levels for the staff to understand what some of the variables that are reported in the two platforms and as a result they have been able to, both at the national and county level, look at the data through the two systems and compare indicator by indicator, because the two systems have common indicators and it is prudent to ascertain that the data on both platforms is the same.
This anomaly has however been remedied by NASCOP reviewing their data collection tools such courtesy of HealthIT and other partners who have been able to support the tool review process to make sure that the gaps that have been identified between the two systems have been harmonized.
When developing the new tools, NASCOP had a stakeholder’s engagement for them to provide their input as to what they needed captured in the tools. The phase-out of NASCOP’s old tools will probably take 6 months as they have to source additional resources to enable them build and roll-out a new tool and ensure that they have 100% coverage of the facilities receiving the new tool. The change in tools needs to be handled with care, because sending out a new tool changes the reporting platforms at the national level and NASCOP wouldn’t want to be in a situation where one wing of the country is using the old tool and have nowhere to report because of reporting platform changes and the other wing is using the new tool.
After the new tool is out, we will still check if we have been able to capture all the interests and if everything is sitting in at KHIS, we will have a recommendation to drop the older reporting tools”
Once the revised tools are in use and they capture all the information that is both required by all the relevant parties then the journey towards self-reliance will have started in earnest as well as the journey towards having a single source of HIV data in the country. concluded the source

Add a comment